Opioid Hormonal Impact Estimator
Primary Endocrine Risk
Chance of developing hormonal issues.
Specific Side Effect
Expected impact details.
Recommendation:
Enter your dosage to see personalized recommendations based on clinical data.
Enter your daily MME dosage to calculate potential hormonal risks.
You might be taking chronic opioid therapy is a long-term medication regimen for pain management that carries significant endocrine risks because your doctor prescribed it to help you live with less pain. That makes sense. Pain is exhausting, and relief feels like a lifeline. But if you’ve noticed changes in your energy levels, mood, or sex drive that don’t seem to match the rest of your life, there’s a biological reason for it. It’s not just "in your head," and it’s not necessarily normal aging.
Long-term use of opioids disrupts your body’s hormonal system in profound ways. Specifically, these medications suppress the hypothalamic-pituitary-gonadal (HPG) axis is the complex feedback loop between the brain and reproductive organs that regulates hormone production. This suppression leads to a condition known as opioid-induced hypogonadism is a state of reduced sex hormone production caused by prolonged opioid consumption. For men, this often means dangerously low testosterone. For women, it can mean irregular periods, infertility issues, and a loss of libido. The good news? Understanding this link is the first step toward fixing it. You don’t have to choose between pain control and feeling like yourself again.
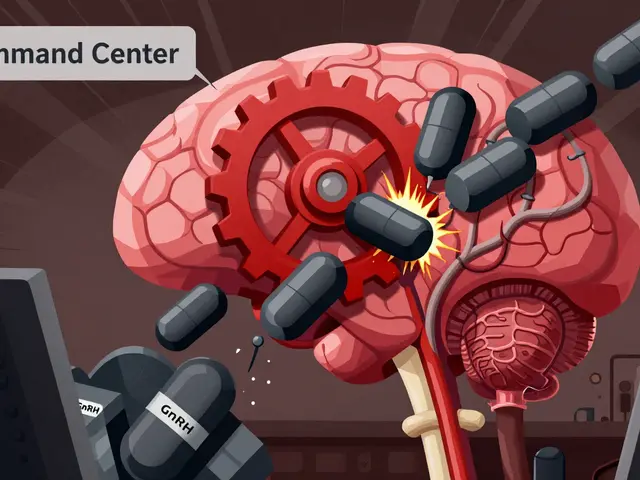
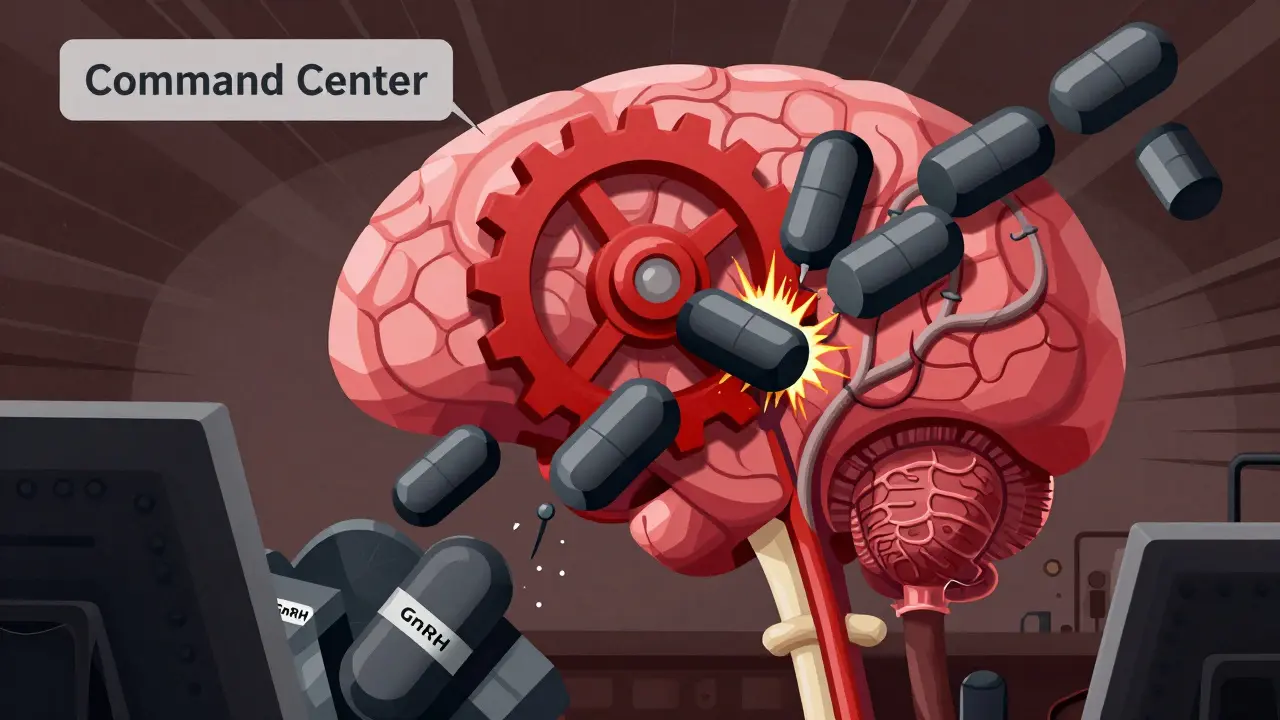
The Biology Behind the Side Effects
To understand why this happens, we need to look at how opioids interact with your brain. Your hypothalamus acts as the command center for your hormones. It releases gonadotropin-releasing hormone (GnRH) is a neuropeptide that triggers the pituitary gland to release luteinizing hormone and follicle-stimulating hormone, which tells your testes or ovaries to produce testosterone or estrogen. Opioids block this signal. They essentially put a dam on the flow of GnRH.
When GnRH secretion drops, your pituitary gland stops producing luteinizing hormone (LH) is a hormone that stimulates the gonads to produce sex steroids. Without LH, your body stops making enough sex hormones. Research published in the Journal of Clinical Endocrinology and Metabolism shows that this isn't a rare side effect. In fact, approximately 63% of male patients on chronic opioid therapy develop biochemical hypogonadism. That’s nearly two out of three men. Even more concerning, significant testosterone suppression can occur at doses as low as 120 morphine milligram equivalents (MME) per day. If you are taking higher doses, the risk increases dramatically.
This mechanism was first documented in the 1970s, yet many patients still aren't warned about it. The result is a cascade of symptoms: fatigue, depression, muscle loss, and yes, sexual dysfunction. It’s important to realize that this is a direct pharmacological effect, not a psychological reaction to having chronic pain.
How It Affects Men
For men, the most visible sign of opioid-induced endocrine disruption is a drop in serum testosterone. Studies show that within just 30 days of starting chronic opioid therapy, testosterone levels can decrease by 30-50%. After six months of continuous use, the majority of men fall below the clinical threshold for hypogonadism, which is defined as total testosterone under 300 ng/dL.
What does low testosterone feel like in daily life? It’s rarely just about sex drive, though that is a major component. Many men report:
- Persistent fatigue that sleep doesn’t fix
- Loss of muscle mass despite exercise
- Mood swings, irritability, or increased anxiety
- Erectile dysfunction and reduced libido
- Brain fog and difficulty concentrating
A 2022 thread on Reddit’s r/ChronicPain community highlighted how common this is. One user noted his testosterone dropped to 180 ng/dL after two years on oxycodone. His doctor didn’t test it until he brought up the symptoms. This delay in diagnosis is typical. Many physicians attribute these symptoms to depression or aging, missing the root cause entirely.

How It Affects Women
Women experience different but equally disruptive hormonal changes. While men see a straightforward drop in testosterone, women face a more complex picture. Total and free testosterone concentrations often decrease, but estradiol levels may remain unaffected initially. However, the impact on the menstrual cycle is severe.
Data from the Cleveland Clinic indicates that 87% of premenopausal women on long-term opioids develop menstrual cycle disorders. This includes amenorrhea (the absence of periods) in up to 67% of cases in some studies, and irregular menses in others. Irregular cycles can lead to unexpected pregnancy risks or, conversely, difficulties conceiving when desired. Beyond fertility, many women report a significant drop in libido, worsening depression, and vaginal dryness.
Research gaps exist here. A 2023 systematic review in the Journal of Women's Health found that only 2% of opioid clinical trials include comprehensive female sexual function assessments. This means treatment protocols for women are often less standardized than those for men, leaving many female patients without clear guidance on how to manage these side effects.
| Medication Class | Impact on Testosterone (Men) | Menstrual Disruption (Women) | Primary Mechanism |
|---|---|---|---|
| Opioids is pain-relieving drugs such as morphine, oxycodone, and fentanyl | High (63% develop hypogonadism) | High (87% experience cycle disorders) | HPG Axis Suppression |
| Gabapentinoids is medications like pregabalin used for nerve pain | Low (12% affect levels) | Minimal | Calcium channel modulation |
| NSAIDs is non-steroidal anti-inflammatory drugs like ibuprofen | Negligible | Negligible | Prostaglandin inhibition |
Are There Safer Alternatives?
If you are suffering from chronic non-cancer pain, guidelines from the American Pain Society recommend against using opioids as a first-line treatment precisely because of these systemic side effects. There are alternatives that carry significantly lower endocrine risks.
Gabapentinoids, such as pregabalin or gabapentin, are often used for neuropathic pain. Comparative analysis shows they affect testosterone levels in only 12% of male patients, compared to 63% for opioids. NSAIDs like ibuprofen or naproxen have minimal endocrine effects at standard doses, though they carry gastrointestinal and cardiovascular risks with long-term use. Cognitive Behavioral Therapy (CBT) and physical therapy also demonstrate superior long-term outcomes for many chronic pain conditions without any hormonal side effects.
However, for severe pain-such as advanced cancer or post-surgical recovery-opioids remain clinically necessary. The goal isn’t always to stop them entirely, but to manage the damage they cause. Newer formulations, like buprenorphine buccal film (Belbuca), approved by the FDA in 2023, show 40% lower rates of endocrine disruption compared to traditional full agonists like oxycodone or fentanyl. Discussing these options with your provider is crucial.

Treatment and Management Strategies
If you are already on opioids and experiencing these symptoms, there are evidence-based interventions. The Endocrine Society recommends baseline testosterone testing before initiating chronic opioid therapy, with follow-up testing every six months for men. For women, monitoring menstrual patterns is essential.
Testosterone Replacement Therapy (TRT) is the primary intervention for men. Studies show that restoring testosterone to normal ranges improves sexual function in 70-85% of cases. However, TRT requires careful monitoring due to risks like polycythemia (thickening of the blood) in 15-20% of users. It is not a standalone fix; it works best when combined with pain management adjustments.
For erectile dysfunction, phosphodiesterase-5 inhibitors like sildenafil or tadalafil show 60-70% efficacy. For women, options are less standardized. Some clinicians use off-label testosterone patches (1-2 mg daily), reporting 50-60% improvement in libido in small studies. Another emerging strategy involves combining low-dose naltrexone with reduced opioid dosing. Findings from Cleveland Clinic in March 2024 showed this approach maintained pain control while improving testosterone levels by 25-35% in 68% of patients.
Crucially, never attempt to taper off opioids unsupervised. Withdrawal can be severe, and 73% of patients attempting unsupervised tapering relapse to previous dosing within 90 days. Work with a multidisciplinary team including pain specialists and endocrinologists.
Advocating for Your Health
The biggest barrier to treatment is often silence. Dr. Bolash of the Cleveland Clinic emphasizes that physicians must take the lead in asking about taboo topics like sexual health. But many patients report their doctors dismiss these symptoms as "normal aging" or "depression." You know your body better than anyone. If you notice a sudden change in your energy, mood, or sexual function after starting opioids, bring it up directly.
Ask for blood work. Request a testosterone panel. Ask about alternative pain management strategies. The gap between guidelines and practice is wide; only 38% of primary care physicians routinely screen for opioid-induced endocrinopathy. By advocating for yourself, you bridge that gap. Your quality of life depends on addressing the whole picture-not just the pain, but the person living with it.
How long does it take for opioids to affect hormone levels?
Significant testosterone suppression can begin within 30 days of initiating chronic opioid therapy. However, clinical hypogonadism (testosterone below 300 ng/dL) typically develops after 6 months of continuous use at moderate to high doses.
Can hormone levels return to normal after stopping opioids?
In many cases, yes. Once the opioid is removed from the system, the HPG axis can recover. However, this process can take several months to a year. Some patients may require temporary hormone replacement therapy during the recovery phase to support their body’s natural restart.
Is opioid-induced hypogonadism permanent?
It is generally not permanent if the underlying cause (opioid use) is addressed. However, prolonged untreated hypogonadism can lead to secondary issues like bone density loss (osteoporosis) or muscle wasting, which may take longer to reverse. Early intervention is key.
Do all opioids affect hormones equally?
No. Full agonists like morphine, oxycodone, and fentanyl have the most pronounced endocrine effects. Partial agonists like buprenorphine show significantly lower rates of endocrine disruption, making them a potentially safer option for long-term pain management.
What should I ask my doctor if I suspect opioid-induced hormonal issues?
Ask for a comprehensive hormone panel, including total and free testosterone, LH, and FSH. Discuss your symptoms openly, specifically mentioning changes in libido, energy, or menstrual cycles. Ask if switching to a partial agonist like buprenorphine or adding non-opioid adjuvants could reduce your dose and mitigate side effects.