Lopinavir/Ritonavir Interaction Checker
Imagine taking a powerful medicine that stops your liver from breaking it down. Sounds efficient, right? That is exactly what Lopinavir/ritonavir is a fixed-dose combination antiretroviral therapy where ritonavir inhibits CYP3A4-mediated metabolism of lopinavir to increase its plasma concentration. Also known as Kaletra, this drug was approved by the FDA in 2000 for HIV-1 treatment. It works by using a tiny dose of one drug (ritonavir) to block the enzyme that destroys the main drug (lopinavir). This "boosting" strategy keeps lopinavir in your blood longer and at higher levels. But there is a catch. Because ritonavir blocks the CYP3A4 enzyme is a primary liver enzyme responsible for metabolizing approximately half of all prescription drugs., it also blocks many other medicines you might be taking. This creates widespread and sometimes dangerous drug interactions.
How Pharmacokinetic Boosting Works
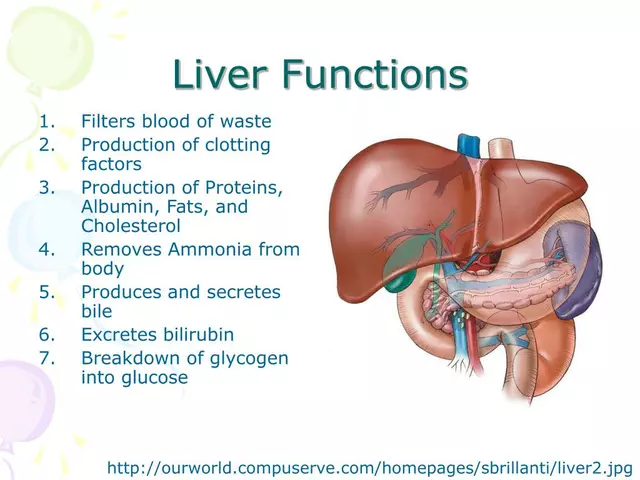
To understand why these interactions happen, you need to look at how your body processes drugs. Most medications are broken down by enzymes in your liver. Lopinavir is no exception. Without help, your liver’s CYP3A4 enzymes would clear lopinavir from your system in about 7 hours. You would have to take it three times a day to keep it working. That is hard for anyone to stick to.
Ritonavir changes the game. It acts as a "mechanism-based inactivator." In simple terms, it doesn't just sit on the enzyme; it effectively breaks it or locks it up so it can't work. When you add just 100mg of ritonavir to 400mg of lopinavir, the metabolic clearance of lopinavir drops by more than 85%. Your liver stops destroying the drug as fast. The result? You only need to take the pill twice a day, and it stays effective longer.
This technique isn't new to HIV treatment. We see similar strategies with cobicistat, another booster used in modern HIV regimens. However, ritonavir is older and behaves differently. While cobicistat is selective-mostly hitting CYP3A4-ritonavir is like a blunt instrument. It hits CYP3A4 hard, but it also affects other enzymes. This lack of selectivity is the root cause of the complex interaction profile clinicians worry about today.
The Double-Edged Sword of Ritonavir
You might think blocking an enzyme is straightforward. If you block the breakdown, drug levels go up. Simple, right? Not with ritonavir. It has a dual personality. On one hand, it is a strong inhibitor of CYP3A4 and CYP2D6. On the other hand, it induces (speeds up) several other enzymes, including CYP1A2, CYP2B6, CYP2C9, and CYP2C19.
This means ritonavir can do two opposite things at once:
- Increase levels of drugs processed by CYP3A4 (like midazolam or fentanyl), potentially leading to toxicity.
- Decrease levels of drugs processed by induced enzymes (like warfarin or methadone), potentially making them ineffective.
For example, if you take warfarin, a blood thinner, ritonavir speeds up its breakdown via CYP2C9 induction. Your INR levels could drop, increasing your risk of clots. Conversely, if you take midazolam, a sedative, ritonavir blocks its breakdown via CYP3A4 inhibition. Your exposure to midazolam can skyrocket by 500%, causing dangerous oversedation. This unpredictability makes managing patients on lopinavir/ritonavir a constant balancing act.
| Drug Class | Example Drugs | Interaction Effect | Clinical Action |
|---|---|---|---|
| Opioids | Fentanyl, Methadone | Fentanyl levels rise 300%; Methadone metabolism increases | Reduce fentanyl dose by 60-80%; Increase methadone by 20-33% |
| Sedatives | Midazolam | Exposure increases 500% | Avoid use or reduce dose significantly |
| Blood Thinners | Warfarin, Rivaroxaban | Warfarin levels drop; Rivaroxaban contraindicated | Monitor INR frequently; Avoid rivaroxaban |
| Immunosuppressants | Tacrolimus | Levels rise dangerously high | Reduce tacrolimus dose by 75% |
| Statins | Simvastatin, Lovastatin | Muscle toxicity risk increases | Avoid simvastatin/lovastatin; Use pravastatin instead |

Why Clinicians Are Moving Away from LPV/r
If you walk into a pharmacy in the United States today, you rarely see prescriptions for lopinavir/ritonavir. Why? Because better options exist. Newer integrase inhibitors and boosted protease inhibitors like darunavir/cobicistat offer similar viral suppression with fewer side effects and simpler interaction profiles.
Data supports this shift. A 2022 meta-analysis found that patients on lopinavir/ritonavir discontinued their treatment 37% more often due to adverse events compared to those on newer regimens. Common complaints include gastrointestinal distress, lipid abnormalities, and insulin resistance. Furthermore, the Liverpool HIV Interactions database lists over 1,200 potential interactions with lopinavir/ritonavir, compared to roughly 900 for darunavir/cobicistat.
However, cost matters. In low-and-middle-income countries, lopinavir/ritonavir remains a cornerstone of HIV treatment. It costs about $68 per person per year through programs like PEPFAR, whereas newer agents like dolutegravir can cost nearly five times as much. Until global pricing equalizes, millions of people will continue relying on this older, more complex regimen.

Practical Steps for Managing Interactions
If you or a loved one is prescribed lopinavir/ritonavir, vigilance is key. Here is how to stay safe:
- Screen Everything: Before starting any new medication, supplement, or herbal remedy, check for interactions. Even over-the-counter pain relievers or St. John's Wort can cause issues.
- Use Reliable Tools: Don't rely on memory. Use databases like the Liverpool HIV Interactions database or consult a pharmacist who specializes in HIV care.
- Monitor Levels: If you are on drugs like tacrolimus or warfarin, expect frequent blood tests to adjust doses as needed.
- Watch for Symptoms: Be alert for signs of toxicity (extreme fatigue, confusion, muscle pain) or treatment failure (return of flu-like symptoms, weight loss).
- Consider Contraception: Ritonavir reduces the effectiveness of hormonal contraceptives by up to 50%. Always use backup methods like condoms.
Perioperative settings require extra caution. Anesthesiologists must know if a patient is on ritonavir before surgery. Standard doses of anesthesia drugs can become toxic. Protocols at major health systems recommend reducing opioid and sedative doses by 60-80% to prevent respiratory depression during recovery.
Future Outlook and Alternatives
The role of ritonavir is evolving. While its use in HIV is declining in wealthy nations, it found a second life in COVID-19 treatment. The drug nirmatrelvir (part of Paxlovid) uses ritonavir as a booster to inhibit CYP3A4, keeping nirmatrelvir levels high enough to fight the virus. This proved the boosting concept still has value, even if the specific combination of lopinavir/ritonavir is fading.
Research continues into personalized medicine. Scientists are studying how genetic variations, such as CYP3A5 polymorphisms, affect how individuals process lopinavir. Some people naturally express more of these enzymes, leading to lower drug levels and higher risk of treatment failure. Understanding these genetics could help tailor dosing in the future, making older drugs safer for specific populations.
For now, the message is clear. Lopinavir/ritonavir is a potent tool, but it demands respect. Its ability to manipulate liver enzymes saves lives by controlling HIV, but it also opens the door to widespread drug interactions. Careful management, open communication with healthcare providers, and regular monitoring are essential to navigating this complex therapeutic landscape.
What is the main purpose of adding ritonavir to lopinavir?
Ritonavir is added to lopinavir to inhibit the CYP3A4 enzyme in the liver. This prevents the rapid breakdown of lopinavir, allowing it to stay in the bloodstream longer and at higher concentrations. This "boosting" effect enables less frequent dosing (twice daily instead of three times) and improves overall efficacy against HIV.
Can I take statins while on lopinavir/ritonavir?
It depends on the statin. Simvastatin and lovastatin should generally be avoided because ritonavir significantly increases their levels, raising the risk of severe muscle damage (rhabdomyolysis). Safer alternatives like pravastatin or rosuvastatin may be used with careful monitoring and dose adjustments.
Does lopinavir/ritonavir interact with birth control pills?
Yes. Ritonavir induces certain liver enzymes that break down estrogen and progestin, reducing the effectiveness of hormonal contraceptives by up to 50%. Patients are advised to use additional non-hormonal barrier methods, such as condoms, to prevent unintended pregnancy.
Why is lopinavir/ritonavir less common in the US now?
Newer antiretroviral therapies, particularly integrase inhibitors and darunavir/cobicistat, offer better tolerability, fewer drug interactions, and simpler dosing schedules. Clinical trials show higher discontinuation rates for lopinavir/ritonavir due to side effects like gastrointestinal issues and metabolic changes, leading guidelines to favor newer agents.
How does ritonavir affect anesthesia during surgery?
Ritonavir drastically increases the exposure to many anesthetic drugs, including fentanyl and midazolam, by inhibiting their metabolism. This can lead to prolonged sedation and respiratory depression. Anesthesiologists typically reduce doses of these agents by 60-80% for patients taking ritonavir to ensure safety.